
It’s been a while! And there is a lot to cover, so we’re going to break everything into 3 sections.
1) What is transmission like now?
2) What about Post-COVID-19 Infection?
3) What can we do?
1) What is Transmission Like Now?
A lot has changed since we last looked at numbers. BC no longer offers PCR tests to the general public. PCR testing in BC is now reserved for health care providers, international air travel, and managing care home outbreaks. This has significantly changed our ability to monitor the pandemic! Thankfully, we also started doing viral testing on wastewater at 5 treatment plants, and we still have data on hospitalizations. So let’s take a look at what we have:
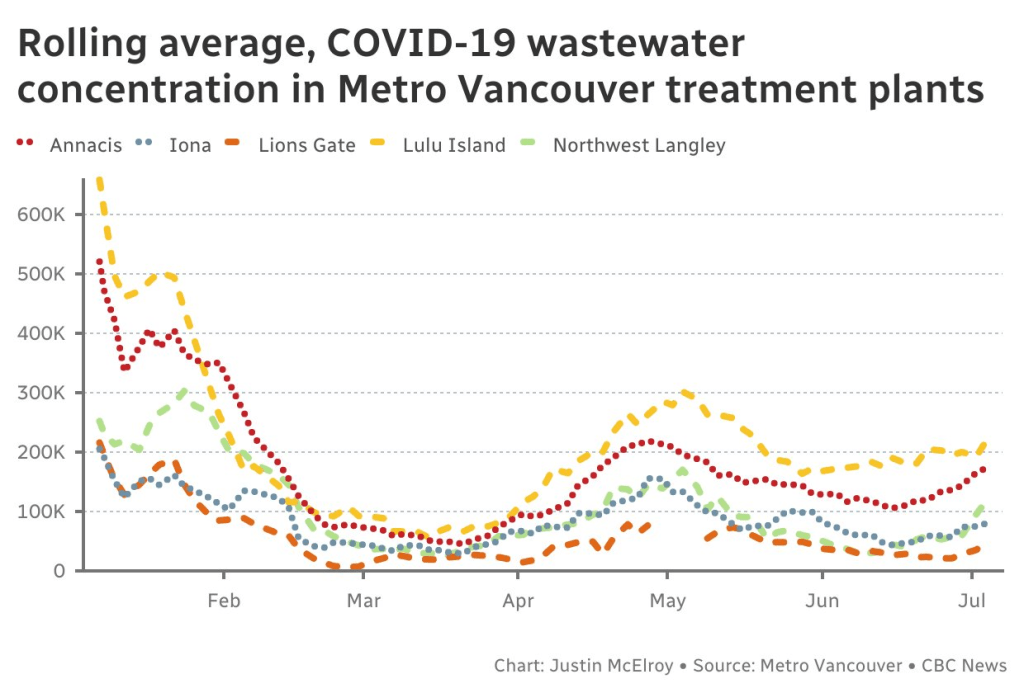
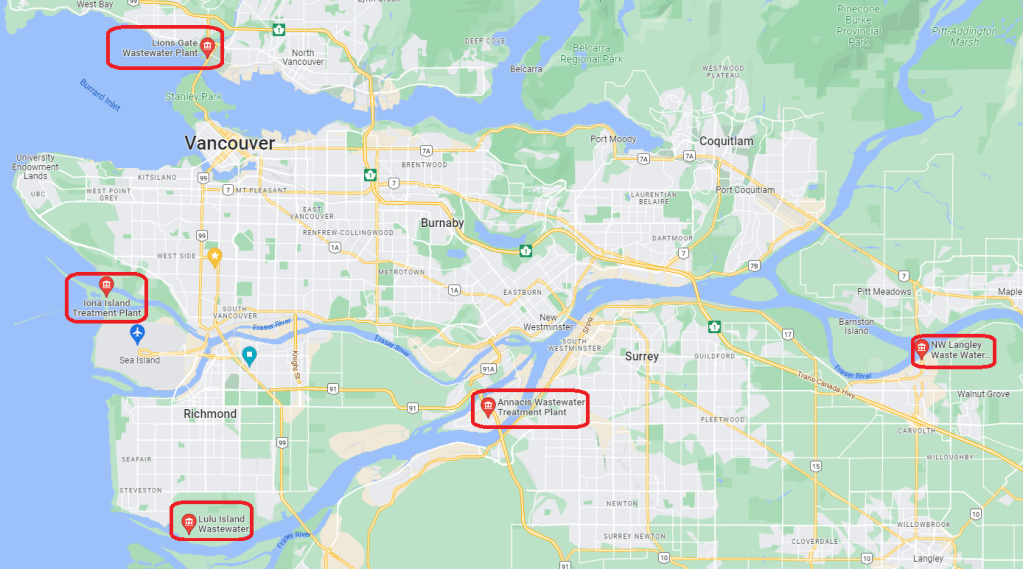
BC has 5 wastewater treatment plants participating in COVID-19 surveillance, which is great as long as you are only looking for data relevant to the immediate lower mainland.
The first thing that stands out is that COVID-19 was detected in massive quantities at the beginning of the year, and nothing we have seen since then has compared. This time frame corresponds to the initial outbreak of the early omicron BA.1 variant in our province. The next major jump in detected COVID-19 samples came in the April-May period, which corresponds with when Omicron BA.2 surpassed BA.1.
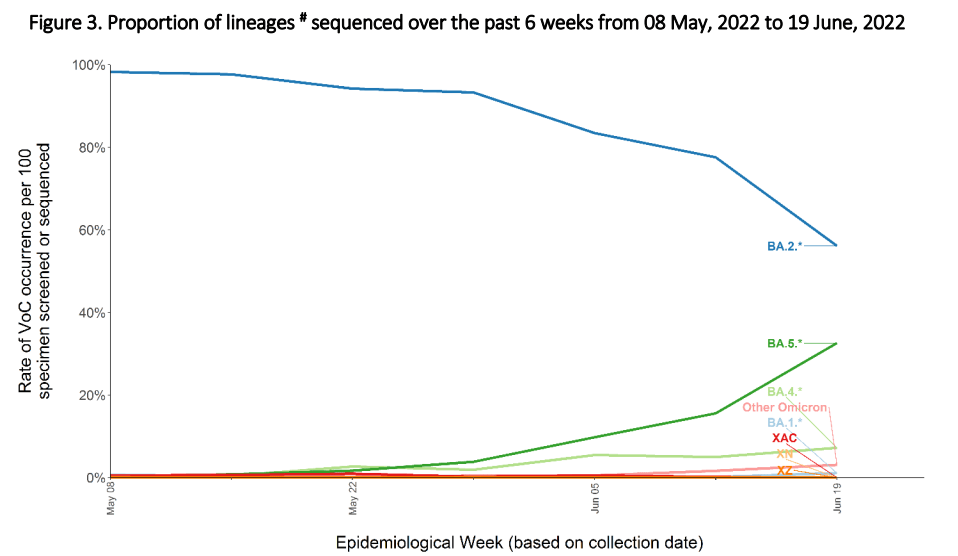
The last 2 wastewater updates have shown us that BC is now headed into a new COVID-19 surge. This also corresponds to BC CDC data showing that the new BA.5 Omicron variant is beginning to replace the previous BA.2 as the dominant strain.

When looking at the above hospitalization data please keep in mind that the lines represent individuals hospitalized who also tested positive for COVID-19, and do not necessarily represent people who are hospitalized due to COVID-19. Since this is one of the few remaining areas where PCR tests are still utilized, this graph can be very helpful in showing current COVID-19 transmission levels across our province.
If you compare the hospitalization graph to the wastewater data graph you will see that all the peaks and valleys relate accordingly, which has been consistent throughout the pandemic so far, but 3 key points of note are important to mention.
Firstly, we have seen the start of a new surge of hospitalizations and increased transmission recently, as the last 2 weeks of reporting have shown significant increases. This new Omicron wave is expected to increase rapidly and peak later in August.
secondly, COVID-19 surges are happening much more frequently now. Previously we saw surges every 4-6 months, but now we are seeing them every 2-3 months.
Thirdly, we are seeing our baseline (non-surge) numbers settle at much higher levels than previously experienced. Specifically, during the April/May surge we saw COVID-19 samples increase between 300-600% from March levels, but after the surge they only dropped by about half. This implies a staggering level of ongoing community transmission even during our “low risk” periods.
But we’re all vaccinated right? So what’s with all the transmission??
The COVID-19 vaccines, like all other vaccines, serve 3 functions. The first function is to reduce infection (and by association, also transmission), but they also reduce the risk of serious disease, and most importantly they serve to reduce the risk of death.
SARS-CoV-2, the virus that causes COVID-19, is an RNA virus. Unlike DNA viruses, RNA viruses are extremely prone to mutations and have the chance of mutating with literally every new infection. As the virus mutates, the new strains that are most able to circumvent protections against infection are the ones most likely to become dominant in any region. The vaccine that has been used up until now has been based on the very early original strains of SARS-CoV-2, and with each major new variant saw reduced efficacy at preventing infection and transmission and shorter and shorter windows after inoculation where that protection functioned. But it is very important to remember that vaccinations are still extremely effective at preventing serious acute illness or death.
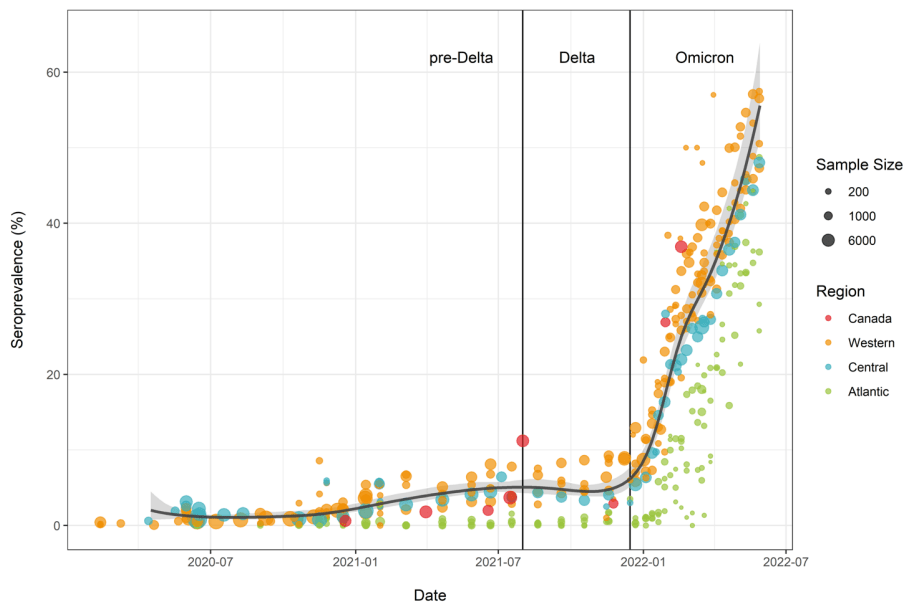
Unfortunately, Omicron has been a pandemic game changer. Since Omicron came to Canada late last year, according to seropositivity testing on a national level, the number of Canadians who have caught COVID-19 jumped from 7% to over 50% between December 2021 and May 2022, and this is especially true of the Western provinces such as British Columbia and Alberta.
So now almost all Canadians are at least double vaccinated and more than half also have caught COVID-19 at least once. You might be thinking about the term “super immunity” that some doctors were theorizing about late last year and early this year. Unfortunately, the studies were primarily based on breakthrough infections with the Delta variant of COVID-19, and we later learned that Omicron can all but ignore immunity gained from previous variant infections.

In fact, we have learned that each new variant of Omicron seems to be better and better at ignoring immunity from previous infections of any variant kind, including itself! But where does this leave us in terms of immunity to new infections? With the current variants BA.4 and BA.5, it appears you can now catch a new infection in as little as 6-8 weeks (note: shorter time frames have been recorded, but those represent extreme and unusual circumstances).

So how common is reinfection? Unfortunately, neither BC nor Canada specifically track that data. The best we can do is look at other places and see how Omicron BA.4 and BA.5 are affecting them. Thankfully, England is doing a very good job of tracking reinfections, and we can see that in the most recent weeks more than 25% of their new infections are also reinfections. Your Local Epidemiologist has also written on the topic of reinfections if you want more information. A recent study on Omicron immunity escape can be found here.

COVID-19 related deaths have been quite high over the course of 2022, but it’s important to remember that close to 50% of all people in BC caught COVID-19 at least once between December 2021 and May 2022, so the percentage of COVID-19 cases resulting in death during the acute phase is actually much lower compared to earlier variants in pre-vaccination times. This is the reason why you might hear Omicron referred to as a “mild” disease, despite the total number of deaths attributed to it being much higher than other variants.
This brings us up to date on everything that has or is currently spreading in BC. But it’s important to keep our eyes on what is happening in the rest of the world since eventually, it will make its way here as well.
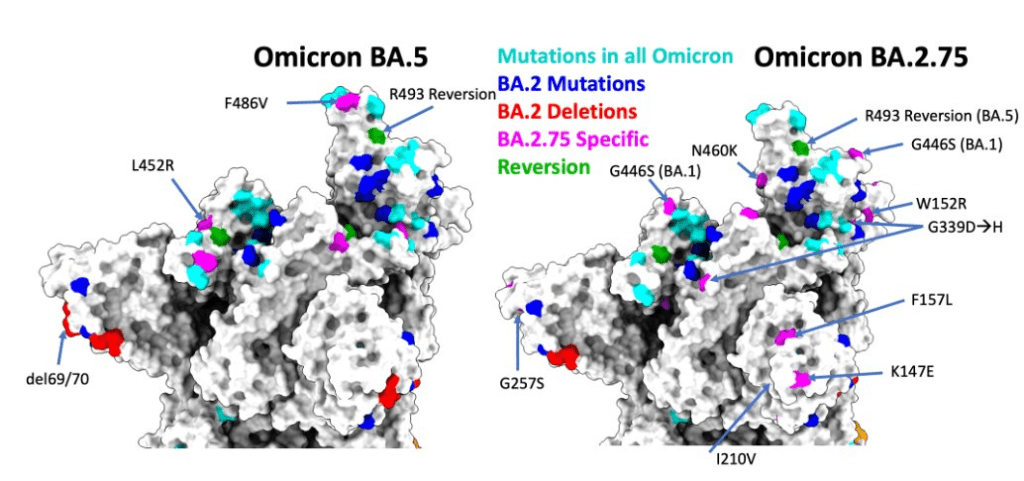
This is Omicron BA.2.75, or as it is colloquially known: Centaurus. Centaurus is a brand new variant that was first discovered in India and has a number of potential genetic advantages over other major COVID-19 variants. We don’t yet know how this will affect transmission rates compared to BA.5, and data sets are still inconclusive. Current data suggest Centaurus could be 2x as infectious as BA.5, and others suggest it could be 8-9x more infectious. We simply need more data. We do know that has already appeared in 10 countries including the US though.
For ease of comparison, Omicron currently is considered to have an r0 value ranging between 9.5 and 23 (in outlier situations). This can be compared to measles which has an r0 of 12-18, and is generally considered the most infectious disease in the world. It is no exaggeration to say that the risk of COVID-19 transmission has never been higher. In fact, one COVID Journalist compared it to a “Forever Plague“.
Note: r0 is the reproduction number of a disease and is based on the number of new infections each infected individual is likely to cause. It is also an estimate, averaged based on available data, and especially for COVID-19, not an absolute consistent value.

The good news is that our vaccinations are still working very hard for us in protecting against serious illness and death from the acute illness phase of COVID-19. This is very important and has been key in keeping our hospitalizations lowered, at least in the short term.
2) What About Post-COVID-19 Infection?
At this point, if you live in BC, most places in Canada, or even most other countries, the odds are that you’ve already had COVID-19 at least once, or possibly 3-5 times even in the most extreme cases (that we are aware of). Chances are even very high that you didn’t even know you had the disease! A meta-analysis of asymptomatic cases published in December of 2021 found that asymptomatic cases could account for 40.5% of COVID infections, and that is not taking into consideration the changes that came with Omicron.
Here in BC, and in many places around the world, the focus has been on reducing serious illness or death from acute COVID-19. That is to say, making sure people are able to survive the infectious period of the disease. And with that goal in mind, BC has been very successful! An individual’s chance of death due to acute COVID-19 is lower now than it has been all pandemic. Unfortunately, we are learning more and more that COVID-19 isn’t just a “survive or don’t survive” event for many people. Even the mildest or asymptomatic cases of COVID-19 can come with long-term health issues in the form of what is often referred to as “Long Covid.”
Long Covid is a kind of catch-all term used to describe the after-effects of a COVID-19 acute infection, due in part to the wide range of potential outcomes, some of which are not even immediately recognizable without specific and expensive testing. Because of this, and the uncertainty created by the high commonality of unreported asymptomatic cases, current estimates place Long Covid as a result in anywhere from 5% to 50% of all acute COVID-19 infections. Health Canada currently says this about Long Covid:
“More recent research shows about 30% to 40% of people who weren’t hospitalized for their initial COVID-19 infection still report symptoms beyond 12 weeks. Current evidence suggests that post COVID-19 condition is higher among those who were hospitalized with COVID-19 compared to those who weren’t hospitalized. This percentage may change as more evidence emerges.”
Unfortunately, recent studies also show that being vaccinated only improves your chances of avoiding Long Covid by about 15%. The W.H.O. also confirmed that the more times a person contracts COVID-19, the more likely they are to end up with Long Covid issues. At this time taking steps to prevent infection is still your best protection against long-term health issues from COVID-19.
Currently, there is a lot we do not know or understand about Long Covid, but every day new information becomes available. A study was published at the end of June 2022 that provides some hope that we may see a test for helping diagnose patients with Long Covid in the near future. The test looks for a reaction from a patient’s t-cells which is a specific response to SARS-CoV-2, and is detectable past the point where infection-induced COVID-19 antibodies can be found. More information can be found here.
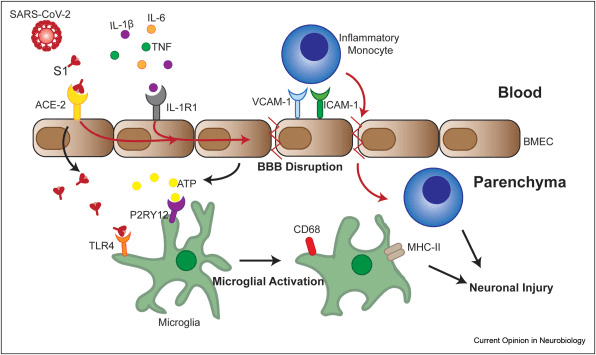
Many patients with Long Covid suffer from neurological conditions. These can range from mild (headaches, difficulty sleeping) to more severe (brain fog, hemorrhages). Currently, there is no consensus on how the SARS-CoV-2 virus can cause this level of brain damage, but one new study suggests it’s related to disruption of the blood-brain barrier. You can also find more theories on the effects of COVID-19-induced neuroinflammation here.
One of the most concerning things we’ve learned about the damage COVID-19 infection does to our bodies is its effect on the immune system. Specifically the damage it can cause to our T-Cells. (T-Cells are an essential part of our immune system and can be broken into different categories, including Helper CD4+ T-Cells, Killer T-Cells, Memory T-Cells, and more. T-Cells also lose their regenerative capacity early into adulthood) Early in the pandemic, it was discovered that patients with severe COVID-19 often suffered from a notable decrease in T-Cell populations, but it was not known if this was caused by the disease, or perhaps was the reason the disease became so severe.
A study published in March 2022 determined that yes, SARS-CoV-2 was directly infecting and killing T-Cells, and unexpectedly, it was doing so without using the spike-protein to ACE2 entry method it’s famously known for. The results heavily suggest that the infection gateway may be LFA-1 (Lymphocyte function-associated antigen 1), which could also explain how other immune cells become infected. While this theory requires additional study to confirm, here is a quote from the study’s discussion section on what they were able to confirm:
“SARS-CoV-2 infection triggered pronounced T-cell death, which potentially contributed to lymphopenia in patients with COVID-19. T-cell infection may also pose profound influences on patients. Infected T lymphocytes not only lost the ability to control viral infection but may also carry viruses to other parts of the body through blood circulation. In addition, this ACE2-independent infection mode may compromise the therapeutic effect of neutralizing antibodies targeting at spike-ACE2 binding. These may synergistically result in more severe infection outcomes in patients with COVID-19.” (click here for the full discussion section)
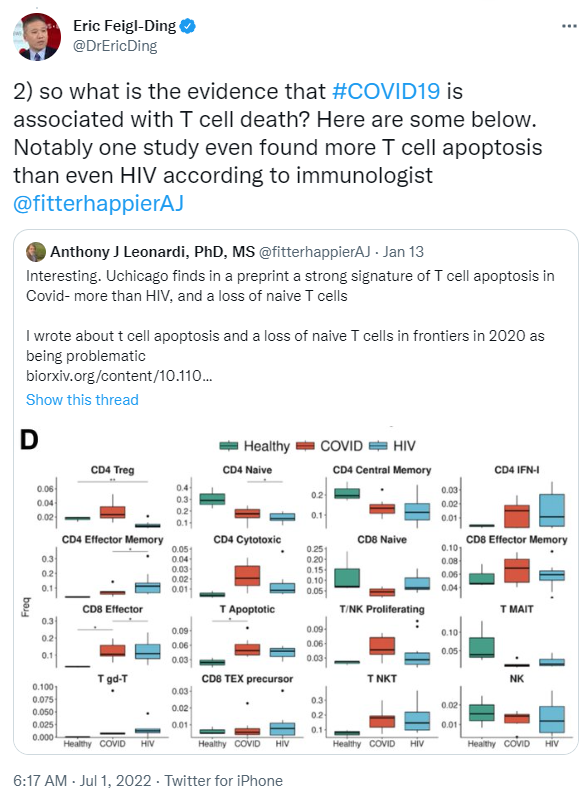


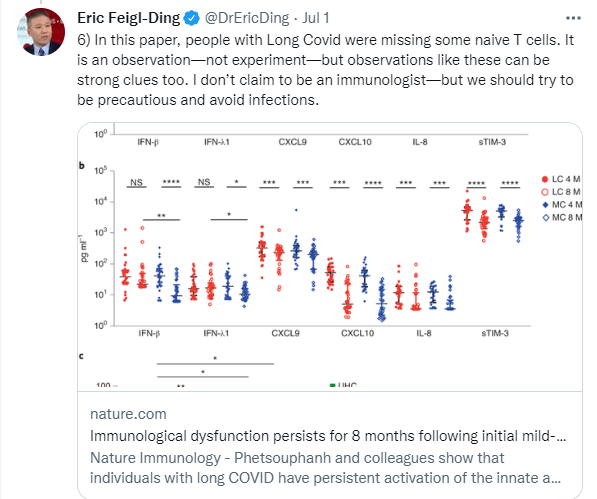
The above screen shots are taken from the Twitter account of Dr. Eric Feigl-Ding, an epidemiologist that has been raising awareness of the long-term immuno-consequences of allowing COVID-19 to spread freely. Here is a link to the thread on Twitter, where you can also find links to all the referenced studies.
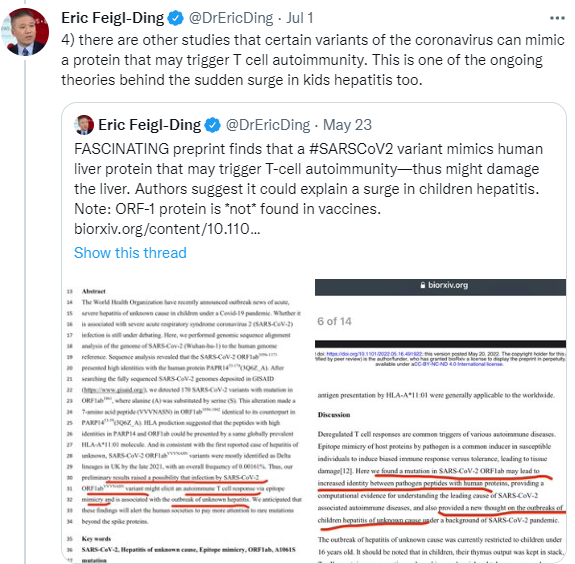
Causing serious damage to our T-Cells isn’t the only way that COVID-19 can affect our immune systems, it has also been known to cause autoimmune conditions. There is also some evidence to suggest that autoantibody responses can be caused by even mild or asymptomatic COVID-19.

Because of the widespread organ and immune damage that COVID-19 can cause, you are also at heightened risk of contracting a number of other diseases, such as:
– Diabetes
– Multiple Types of Heart Disease
– Severe Blood Clotting
– Microclots
– Multisystem Inflammatory Syndrome
– Shingles
Unfortunately, much like how the early stages of cancer can come with no outward warning symptoms, it’s also entirely possible to have a severely compromised immune system and not know it, until it becomes a threat to your health. The very best thing you can do is try to prevent catching COVID-19 entirely.
So what happens if you catch COVID-19 multiple times?
Initially, it was believed and expected that your body would perform better against COVID-19 on each subsequent infection, and perhaps you wouldn’t even notice them eventually. But as the virus mutated, and as we learned more about it, it became clear that the opposite situation was more likely.
A pre-print study (not yet peer-reviewed) was posted in June 2022 that provided compelling evidence that the damage caused by COVID-19 actually stacks with each new infection.
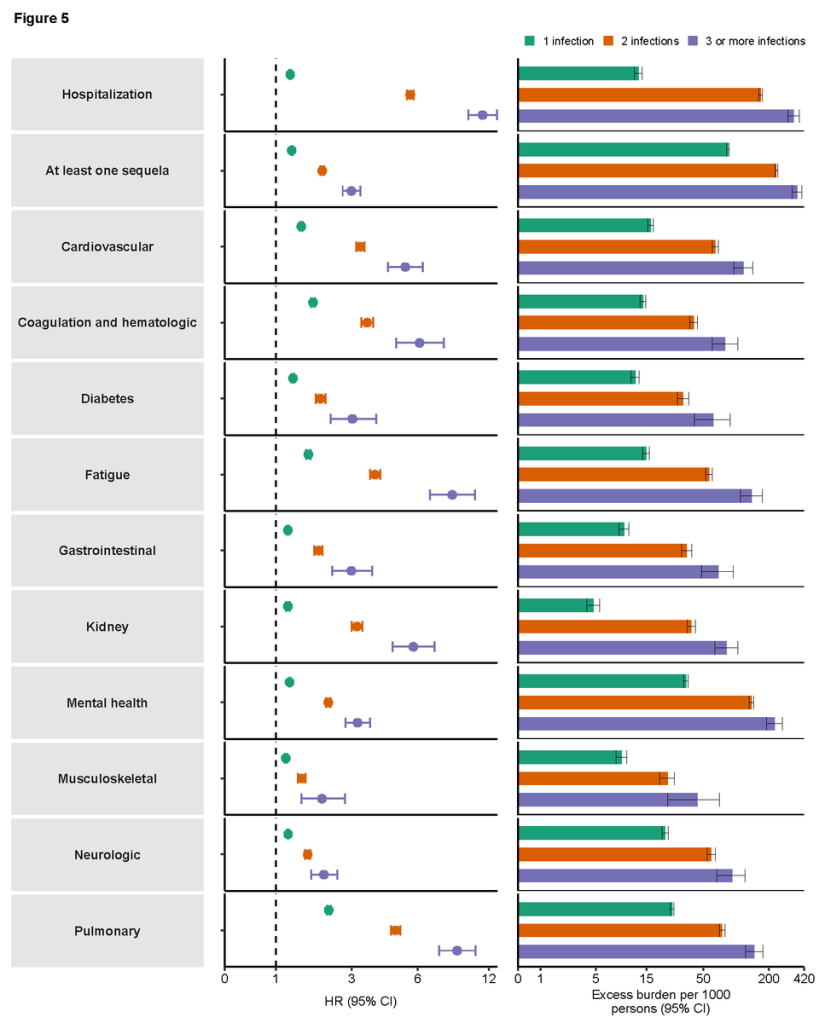
As you can see from the above chart, the hazard ratios increase significantly with each new infection. It is important to remember that this is still just one study, and again, it is not yet peer-reviewed. However, one probably shouldn’t need a lot of convincing that catching COVID-19 multiple times is a bad idea.

Watching the excess death rate of BC against the reported COVID-19-related deaths is another way we can estimate the effect of the disease on immune systems. As you can see, both lines have related to each other for the most part, outside of the heat dome in late June 2021. But from that point onward there has been a large volume of excess deaths beyond the ones marked as COVID-19 related. Of course, we have no way to confirm if these are in any way related to conditions caused or exasperated by Long Covid, it is certainly an area to pay attention to. You can find national data on excess deaths here. It’s also worth mentioning that one of the leading theories on why Alberta’s #1 cause of death in 2021 was “unknown” is because of post-covid complications.

Here you can see the number of deaths reported in BC, broken down by weekly totals for each year. Starting with 2019, each following year shows a substantial increase in deaths in almost every week respective to each year (even ignoring the heat dome), especially in the latter half of each year. It is very concerning to consider the possibility of this trend continuing. (Source)
3) What can we do?
We already know the very best ways to keep ourselves safe in this pandemic. They are the tried and true methods that have already proven effective, and they’ve never been more important than they are now:
- If you haven’t received your 2 vaccine doses and at least 1 booster shot, get that as soon as possible
- As of this week, anyone 18 or over may now request a 2nd booster shot at their discretion. BC Public Health “doesn’t recommend it” at this time, but if you “have unique needs” you can follow this link and click on “I don’t want to wait for the fall” for information on how to request it.
- Wear an N95 or similarly rated mask whenever you are indoors. Wear it over your nose and chin. Don’t “just take it off while I’m talking” or “not put it on because I’m just running to the washroom”.
- Keep your exposure opportunities low. Don’t attend large indoor events every other day. Try not to attend events that don’t mandate mask-wearing and details about air ventilation and/or filtration.
- When possible, meet people outdoors.
- Do your best to stay informed.
Those are all the basics that we’re all used to by now. But there’s more you can do if you feel you want to do more:
(Warning: The following content is largely the opinion of the author, so take it with a grain of salt please)

Buy a C02 monitor and check it periodically when you attend indoor events, to help track how well the air is being ventilated and refreshed. You might be shocked by how bad the ventilation is at some venues, and the only way we can make change happen is by raising awareness of the problem.
When you see indoor events that you want to attend that don’t have reasonable COVID-19 safety policies (or any at all) contact them and let them know it makes you uncomfortable. Many of these events are simply following the minimum set of requirements from BC Public Health, and they don’t understand the level of risk they impose on their attendees because of their lack of safety protocols.
Write to the BC Minister of Health, Adrian Dix, and let him know that you are not satisfied with the policies that have led to the level of transmission of COVID-19, the mass disabling of healthy individuals, the extenuating harm caused to the immuno-compromised, and the high number of related and indirect deaths.
COVID-19 has been rough. It started hard, and it only became more difficult as time went on. But we have to keep doing our best, and trying to make a difference. It might be tempting to give in to the desire to believe that “safety measures don’t make much difference”, or that “everyone is going to get COVID anyways, so it doesn’t matter if you throw a big party and nobody wears masks”. It’s easy to give in to that sweet denial for a sense of justification for poor choices. But it’s not worth it. If you think you’re only risking yourself, you’re also risking your loved ones. If you think you’re only risking the people that attend your event, you’re also risking your friends in common. You can’t designate a section of a public pool for peeing in and expect it to not contaminate the whole space eventually. When your neighborhood is home to coyotes, you keep your outdoor cats inside no matter how much they want to go out and have fun, even if they don’t understand.

But there’s good news! There IS some light at the end of this tunnel. We may have no idea how long COVID-19 will be a major issue in our lives, but we CAN fight back! With SCIENCE! And Science has a couple of doozies coming up for us soon!
Firstly, for the parents of young children out there, we should see vaccinations become available for kids under 5 years old, sometime in the next few weeks!
Secondly, coming this Fall we will be seeing a new vaccine option from Moderna and Pfizer/BioNTech. This bivalent vaccine will include the original formulation we have previously received, as well as an update based on the Omicron BA.1 and BA.2 variants. While this might seem like a “too little too late” situation since BA.1 and BA.2 have already been replaced by BA.4 and BA.5 for the most part, don’t forget that BA.2.75 is a sub-lineage of BA.2. So there is every reason to believe that this new vaccine will offer solid protection against that variant as well (and we know it also works on BA.4 and BA.5, just not quite as well). So we just need to manage a little longer until that becomes available, and we should see a major drop in transmission again.
Thirdly! It is looking very likely that the US will be getting a DIFFERENT version of the new vaccine than we are! Currently, the FDA is leaning heavily toward approving a new vaccine based off of the BA.4 and BA.5 variants. This means that if we find later variants split off from those versions of Omicron, there will already be a vaccine in production that will be fast for us to be able to approve (or individuals can travel South for a shot potentially). At the very least, it’s an option. (more information available here)

And FINALLY! BioNTech and Pfizer have begun work on what they are calling a universal vaccine for coronaviruses! This vaccine would be geared to primarily guard against severe illness and death, and would potentially work against SARS-CoV-1, SARS-CoV-2, MERS-CoV, and even a handful of viruses that make up the common cold.
Ok, that’s it, you made it to the end!
Author’s note:
I started this website more than 2 years ago to help keep track of what it was like to deal with an unprecedented pandemic as it was happening. Over the last 845 days, our province has gone through many changes in trying to adapt to the current situation, from recognizing the virus’s spread to shutting down non-essential businesses, to rolling out a new vaccine, and now, trying very hard to ignore that we have been unsuccessful in eradicating the virus despite all the efforts. During this time I went through some changes as well, from losing my employment, to gaining new employment, to nearly dying during the heatwave of June 2021 and being hospitalized for newly diagnosed diabetes, and more recently contracting COVID-19 in January 2022. I did not expect to be writing here again, and I didn’t really expect there to be a need for me to write here again after vaccinations rolled out! But things don’t always go the way we hope, and here we are. At this time I can’t commit to making more posts on any kind of a regular basis. My decision to make this post today is largely due to how much important information is coming from the scientific community, that is just not being shared either by the media or even by public health. Hopefully, you find this post informative and helpful! And hopefully one day we can put all of this behind us.
-Gregory Neher

Thanks Greg! Welcome back, I have truly missed your reporting. Lots of incredible info in this report. Take care and stay safe.
Sent from my iPhone
LikeLike
Thanks for all this info! It’s good to be prepared.
LikeLike
Thanks Greg for all the updated information…i have missed your reports. Its awesome to have all this information to keep you and all of us safe. Be safe!
LikeLike
I agree with everyone else – your reports were definitely missed.
Thanks for this very useful update.
LikeLike